
Playful Sincerity
Introducing Dialectical Play Therapy

Hi! I’ve been getting assigned a ton of adolescent patients and groups at my work because I’m getting decent feedback and results. Since many of my colleagues run into obstacles with this population I have been asked to develop a training. I wrote this essay in preparation for that training…
I know that not all of us here are in a context where we’re treating adolescent patients, but we might have children in our lives and or want to give attention to an inner child.
When Teenagers Hate Therapy (And What I Do About It)
I'm going to start with a scene that every therapist who works with adolescents knows by heart.
"Tell me about your relationship with food."
The sixteen-year-old across from me—let's call her Maya—rolls her eyes so hard I'm worried they might get stuck. She pulls out her phone. Mutters "fine" in that particular way teenagers have perfected that means absolutely anything but fine.
I'm sitting there feeling like an idiot. This is my third session with Maya, and we're nowhere. Her parents are paying good money for her to stare at TikToks while I ask increasingly desperate questions about her eating disorder. I can feel myself getting that familiar therapist panic—the one where you start wondering if you're actually helping anyone or just collecting copays while kids get sicker.
If you've worked with teenagers for more than five minutes, you know this dance. We push for emotional depth. They retreat into silence or that maddening teenage compliance where they give you just enough to get through the session. We call it resistance. Or if we’re in a more progressive milieu possibly ambivalence. Whatever we call it, the patient experiences it as us being completely disconnected from their reality. We can’t help if we’re not connected.
I spent years in this frustrating loop before I figured out something that changed everything. It's not a technique, exactly. It's like a combo of techniques, framing, and general mindset.
Brains and Safety
Here's what I wish someone had told me in graduate school: when you ask a traumatized seventeen-year-old to "tell me about your family dynamics," you're essentially asking their nervous system to trust you before you've signaled that you're safe.
Think about it. Most therapy starts at what I call intimacy level eight out of ten. "Tell me about your trauma." "How does your depression feel?" "What's your relationship with your parents like?" For an adult who's chosen to be there and has some practice with emotional language, this might work.
For a teenager? It's like asking someone to jump off a cliff before they know if you're there to catch them.
I learned this the hard way through years of failed sessions and kids who never came back. But I also learned it through my own experience as a young person who desperately needed help but couldn't access it through traditional means.
When I was in my late twenties, I started having terrible nightmares. I'd recently come back to the States after working in the Caribbean boating industry, and something in my psyche was unraveling. I ended up in Jungian analysis, not because I knew anything about Jung, but because someone told me that bad dreams were Jungian territory.
My analyst, Stan Marlan, never started our sessions by asking me to explain my trauma or analyze my childhood. He started by meeting me where I was. We talked about the dreams, yes, but also about boats and the ocean and practical things that mattered to me. The deeper work emerged naturally from that foundation of safety.
That experience taught me something crucial: people heal when they feel met, not when they feel analyzed.
What I Call "Playful Sincerity"
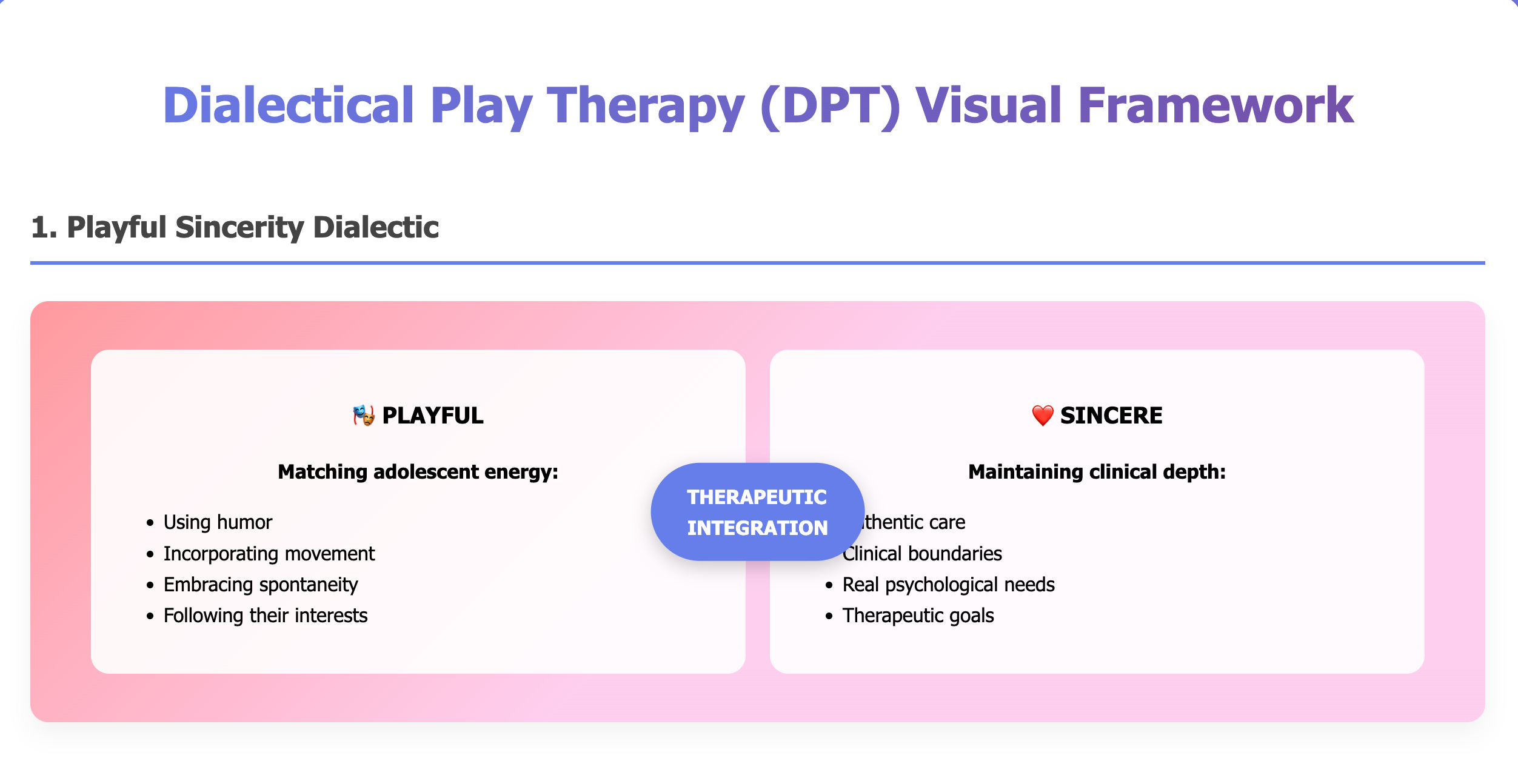
So here's what I do differently now. I've developed what I call a "playful sincerity" approach. It sounds contradictory, but bear with me.
Playful means I match their energy. I notice Maya's cool nail art and ask about it. I comment on the band t-shirt. I'm genuinely curious about their world—trends, school drama, whatever they're actually thinking about.
Sincere means I never lose sight of why we're here. I'm not trying to be their friend. I'm holding space for real psychological work. But I'm doing it in a way that doesn't immediately trigger their defenses.
The magic happens in the integration. I can laugh with you about some ridiculous thing that happened at school AND hold space for the fact that you're struggling with depression. These aren't opposites. They're complementary.
With Maya, instead of diving straight into food and body image, I started noticing things. "That's really intricate nail art—did you do that yourself?" We spent ten minutes talking about nail art techniques. Then, "I'm wondering if you're as creative with other things in your life as you are with your nails. Sometimes creativity shows up in unexpected places."
Notice what I'm doing here. I'm building connection first. I'm honoring her actual interests. And I'm creating a bridge to deeper material without demanding vulnerability she's not ready to give.
The Match+1 Rule
I've developed what I call the Match+1 rule for building intimacy with adolescents. Most therapy tries to jump from zero to sixty. I move in much smaller increments.
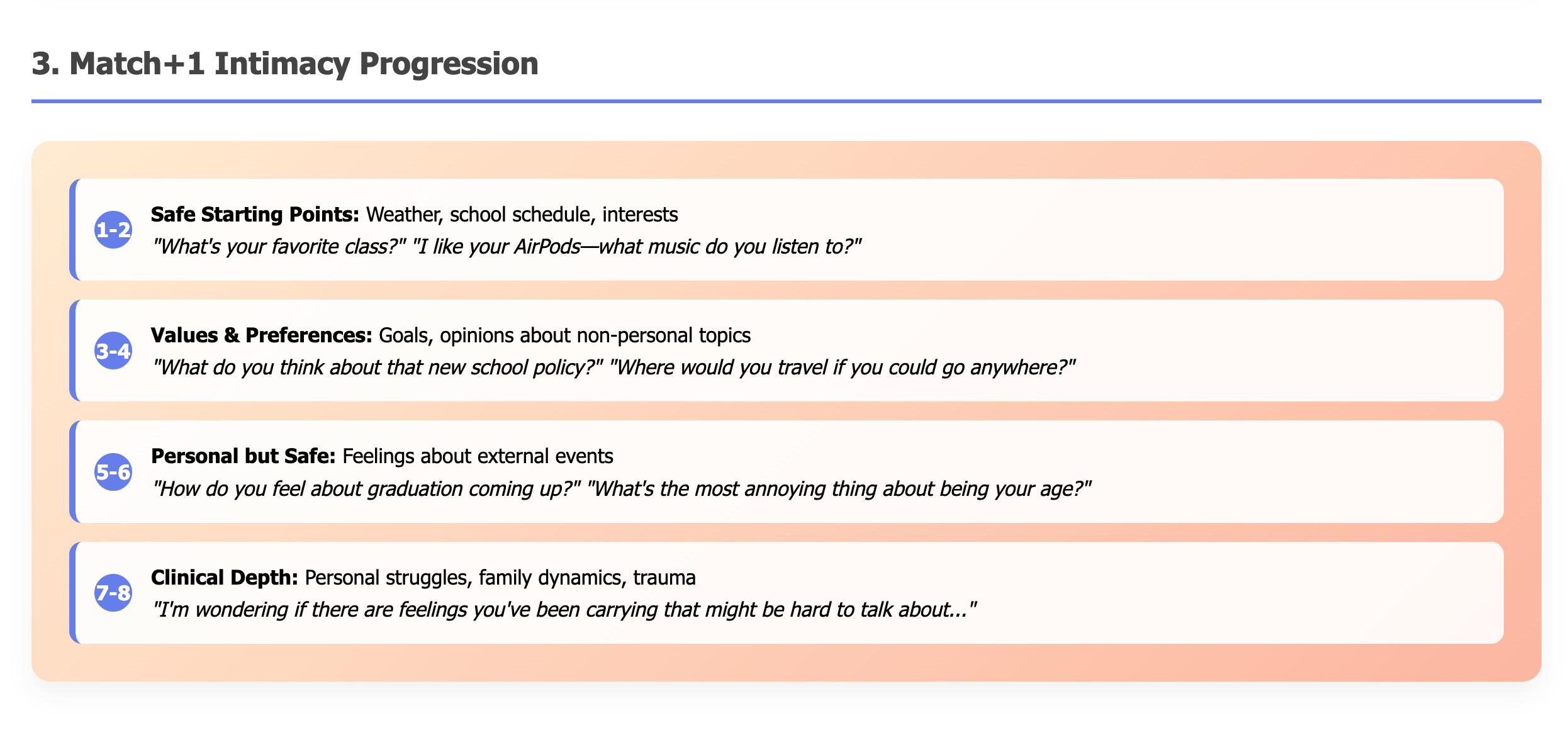
Level 1-2 conversations are about safe stuff. Weather. School schedule. "What's your favorite class?" "I see you have AirPods—what are you listening to?"
Level 3-4 gets into preferences and opinions about non-personal topics. "What do you think about that new school policy?" "If you could travel anywhere, where would you go?"
Level 5-6 starts to get personal but still feels safe. "How do you feel about graduation coming up?" "What's the most annoying thing about being your age?"
Level 7-8 is where the real clinical work lives. "I'm wondering if there are feelings you've been carrying that might be hard to talk about."
The key is matching their current level and then going just one step deeper. Not three steps. Not five. One.
Here's how this played out with Maya:
Session 1: We talked about nail art and her favorite Instagram accounts.
Session 2: She mentioned being stressed about college applications. I asked what felt most overwhelming about the process.
Session 3: She said she felt like she had to be perfect at everything. I wondered aloud if that pressure showed up in other areas of her life.
Session 4: She brought up how she'd been skipping lunch because she felt anxious about eating in front of people.
See what happened? We got to the clinical material, but we got there through a path that felt natural to her. She controlled the pace. I provided the scaffolding.
Countertransference
Here's something I noticed: half of adolescent therapy happens in your own head, managing your reactions to their behavior.
When Maya rolls her eyes for the tenth time, my gut reaction is "She doesn't like me." When that seventeen-year-old gives me one-word answers, I think "I'm failing as a therapist." When they seem bored, I assume "They're not trying."
This is classic countertransference, and with teenagers, it's absolutely toxic to the work.
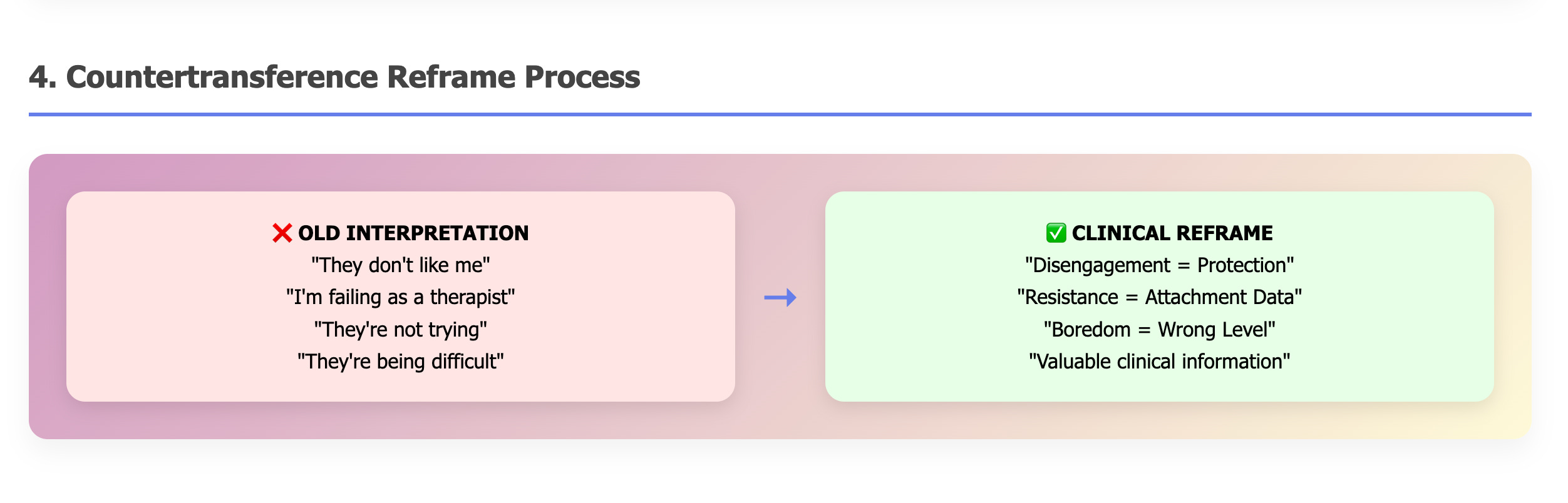
The breakthrough came when I learned to reframe these reactions completely:
Old interpretation: "They don't like me" → Clinical reframe: "Their nervous system is saying this feels too intense too fast"
Old interpretation: "I'm failing as a therapist" → Clinical reframe: "I'm operating at the wrong developmental level"
Old interpretation: "They're not trying" → Clinical reframe: "This is valuable attachment information about how they've learned to protect themselves"
When I notice myself working harder than my client, that's not a sign that I need to push harder. It's clinical data telling me I need to step back and match their developmental level.
This reframe changed everything. My frustration became useful information instead of just frustration.
Neuroscience & and Development
There's real science behind this approach, and it starts with understanding that adolescent brains are basically under construction.
Attachment theory tells us that playfulness signals safety to the nervous system. When I'm genuinely curious about Maya's nail art, I'm sending a message to her limbic system that I'm not a threat.
Polyvagal theory reminds us that we need engagement before we can do therapeutic challenge. You can't process trauma when your nervous system is in protection mode.
But here's what really shifted my understanding: adolescents exist simultaneously across multiple developmental levels. Maya might be cognitively sophisticated enough for AP classes while being emotionally overwhelmed by basic feelings. She might navigate complex social relationships while thinking about family dynamics in very black-and-white terms.
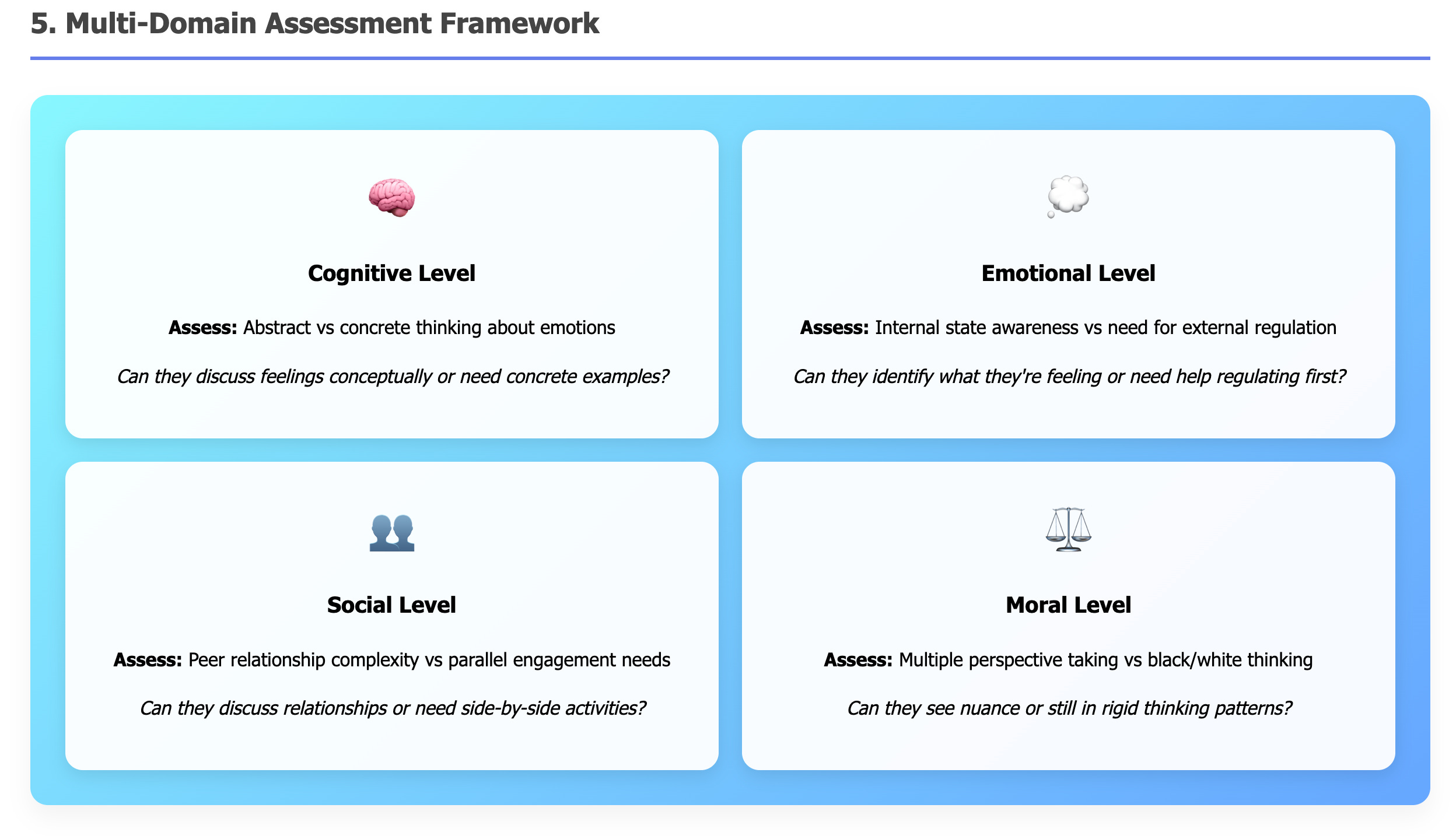
Before I choose any intervention, I assess four domains:
Cognitive Level: Can they think abstractly about emotions, or do they need concrete examples?
Emotional Level: Can they identify what they're feeling, or do they need help regulating first?
Social Level: Can they discuss peer relationships, or do they still need parallel play approaches?
Moral Level: Can they see multiple perspectives, or are they stuck in rigid thinking?
This assessment prevents the mistake I used to make constantly—assuming that because someone is seventeen and articulate, they're ready for the same emotional processing as an adult in therapy.
Scaffolding
Here's the concept that transformed how I think about adolescent therapy: scaffolding.
In education, scaffolding means providing temporary support structures that help students reach higher levels of understanding. You give them just enough support to succeed, then gradually remove that support as they develop competence.
In therapy with adolescents, scaffolding means meeting them at their current developmental level and then building upward in manageable increments. Not jumping from their level to where I think they should be, but creating a bridge they can actually cross.
Most traditional therapy assumes that if someone is cognitively mature enough to understand abstract concepts, they're emotionally ready to process complex trauma or family dynamics. But development doesn't work that way. A seventeen-year-old might have the vocabulary to discuss depression while lacking the emotional regulation skills to actually process those feelings without becoming overwhelmed.
The scaffolding approach recognizes these developmental gaps and works with them instead of against them.
The scaffolding process looks like this:
Here's the step-by-step process I use:
Step 1: Assess their current functioning level across those four domains. I'm watching: Can they think abstractly about feelings? Do they seem regulated or dysregulated? Are they socially sophisticated or do they need more parallel approaches? Are they thinking in black and white or can they see nuance?
Step 2: Meet them at that level to build safety. If they're thinking concretely, I use concrete examples. If they're dysregulated, we do regulation activities before any emotional processing. If they're socially anxious, we might work side-by-side rather than face-to-face.
Step 3: Scaffold up gradually when they're regulated and engaged. This is where the Match+1 rule comes in. I move one step deeper in intimacy, one level higher in complexity, one degree more challenging. Not three steps. One.
Step 4: Drop back down if overwhelm occurs. This is crucial. When I see signs of nervous system activation—they get quiet, fidgety, start looking at their phone, give shorter answers—I immediately drop back to a safer level.
This isn't linear. We might scaffold up and down multiple times in a single session. The key is staying responsive to their cues rather than sticking to my agenda.
What this meant for Maya: instead of asking her to analyze her relationship with food (level 8), I started by noticing her nail art (level 1), moved to asking about her creative interests (level 3), then wondered if creativity showed up in other areas of her life (level 5), and only then approached how she thought about eating (level 7).
Practice
Let me give you some concrete examples of how this plays out with different types of interventions.
Movement-based techniques: Instead of having them sit still and "process feelings," I might suggest we take a walk if they seem restless. Or I'll teach them breathing techniques that involve arm movements. For kids with trauma or ADHD, their bodies often need to move before their minds can settle.
Art and creative work: I keep art supplies in my office. Not because I'm an art therapist, but because sometimes it's easier to show me what anxiety looks like in colors than to try to find words for it. Maya started drawing these intricate patterns while we talked. Turned out they were visual representations of her anxiety—the more chaotic the pattern, the more overwhelmed she felt.
Games and activities: I've got Jenga blocks with different emotions written on them. When someone pulls a block, we talk about that feeling. It sounds silly, but it creates enough distance from the emotion that kids can actually engage with it. I've learned more about teenagers' inner worlds through "therapeutic Jenga" than through years of direct questioning.
The key is that all of this connects back to real therapeutic goals. I'm not just entertaining them. I'm creating multiple entry points for the actual work.
When I Know It's Working
I had a breakthrough moment with a seventeen-year-old who'd been through three previous therapists. Traditional therapy lasted exactly two sessions each time. His parents were frustrated. He was frustrated. Everyone had labeled him "resistant to treatment."
I started by talking about music. He was into this indie rock band I'd never heard of. Instead of pretending to know them, I asked him to teach me about what he liked about their sound. We spent sessions two through four gradually connecting his love of lyrics to emotional expression.
By session eight, he brought in lyrics he'd written about feeling "stuck between frequencies"—unable to connect with anyone around him. We used that metaphor to explore his depression and social anxiety. By month six, his mood had stabilized, his family relationships had improved, and he was actually enjoying school again.
The breakthrough wasn't any single technique. It was meeting him in his world first, then creating a bridge to the work he needed to do.
What Doesn't Work
I need to be clear about when this approach isn't appropriate. If someone is actively psychotic or in immediate danger, you obviously can't spend weeks building rapport through music discussions. Sometimes crisis intervention requires direct, immediate clinical action.
But for the vast majority of adolescent therapy—kids with depression, anxiety, eating disorders, family conflicts, identity issues—this developmental approach transforms the work.
I've seen my therapy dropout rate go from about sixty percent to less than fifteen percent. Alliance building that used to take two months now happens in three weeks. But more importantly, the work goes deeper because the foundation is stronger.
What I Wish I'd Known Earlier
If I could go back and tell my younger therapist self one thing, it would be this: stop trying so hard to be "therapeutic" and start trying to be genuinely curious about the person sitting across from you.
Teenagers can smell therapeutic technique from a mile away. They've been in school for twelve years. They know when an adult is following a script versus when someone is actually interested in them as a person.
The best clinical work I do happens when I forget about being clinical and just get curious. What's it like to be sixteen in 2025? What does their social world actually look like? What are they worried about? What makes them laugh?
When you start there, the clinical material emerges naturally. And when it emerges naturally, they're much more willing to engage with it.
For the Therapists Reading This
If you work with adolescents and you're feeling frustrated, burned out, or like you're not making a difference, I want you to try something with your most challenging client.
Don't ask them about their trauma or their family or their mental health symptoms. Ask them about something they're wearing. Ask about their phone case. Ask what they're listening to. Spend a whole session just being curious about their actual world.
Notice what happens. Notice how they respond when you meet them where they are instead of where you think they should be.
This isn't about becoming less clinical. It's about being clinical in a way that actually works with adolescent development. We're not abandoning the real work—we're creating the conditions where real work becomes possible.
Where This Goes Next
I'm writing this because I think we need to fundamentally rethink how we approach adolescent mental health. Too many kids are falling through the cracks not because they don't want help, but because we're offering help in ways that don't make sense to their developing brains.
Every time you choose curiosity over confrontation, every time you match their developmental level instead of demanding they meet yours, every time you build safety before asking for vulnerability—you're participating in a quiet revolution in how young people experience mental health treatment.
The teenagers in our offices aren't resistant. They're not difficult. They're appropriately protective humans trying to navigate an incredibly complex world. They deserve therapists who can meet them there.
What's been your experience working with adolescents? Have you found approaches that work when traditional therapy doesn't? I'd love to hear your stories.
About me: I'm an eating disorder therapist in Pittsburgh who stumbled into working with teenagers and discovered they're actually the best clients once you figure out how to speak their language. I write about therapy, psychology, and the messy process of helping people.
This was insightful and informative. All vision may rely on the interdependence of an internal and external source. An external image projected in the mind, an internal image projected on our surroundings, and what can be generated from the overlapping of these forms of vision, allows us not just to witness and be witnessed by the world, but reify our beliefs, our dreams, and other visionary forms of the divine and transcendent into an observable imaginary. What truly separates us from our environment or from each other, with those cellular membranes so small and infinite? If immanence is an inward-moving version of transcendence, how does this complicate our understanding of the lyric, and via the lyric, the world?
Good, and evocative write
Wonderful piece, Brian. Resonated with my own experience as well as with my work with kids I saw in my school psychologist work.